


What is Inverted-V Deformity? Defining a Post-Rhinoplasty Challenge
The Inverted-V Deformity is an aesthetic and functional challenge that can emerge after rhinoplasty, characterized by a distinct shadow on the middle third of the nose. It signifies a structural collapse in the nasal midvault, often becoming apparent several months following the initial surgery. This condition is not merely a cosmetic imperfection; it frequently compromises nasal airflow, leading to significant functional impairment. Many mistakenly perceive it as solely a “bad nose job,” overlooking its deeper anatomical and physiological implications.- Visual Cues: A prominent inverted ‘V’ shaped shadow or indentation on the nasal dorsum, particularly noticeable when viewed from the front.
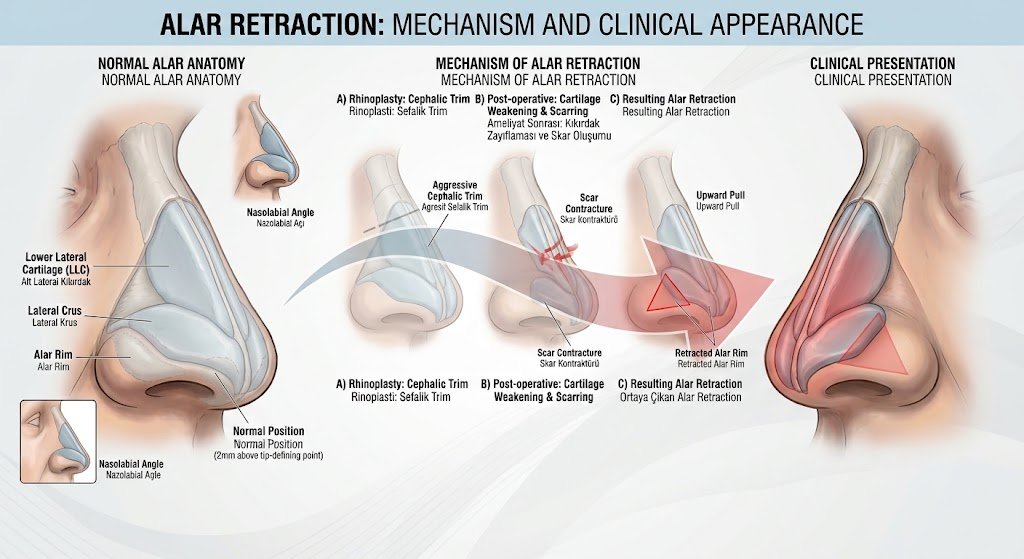
- Anatomical Origin: Occurs due to the collapse of the upper lateral cartilages, which form the middle vault of the nose, often exacerbated by the prominence of the lower edges of the nasal bones.
- Functional Effects: Leads to narrowing of the internal nasal valve, causing nasal airway obstruction and difficulty breathing.
The Anatomy Behind the Deformity: How Cartilage and Bone Interaction Leads to Inverted-V
The nose’s structural integrity relies on a delicate interplay between its bony and cartilaginous components, specifically the nasal bones, upper lateral cartilages, and the nasal septum. The middle nasal vault region, formed by the upper lateral cartilages articulating with the septum and nasal bones, is crucial for both aesthetic contour and functional airflow. During rhinoplasty, particularly dorsal hump reduction, the connections between these structures can be disrupted. The precise balance between the upper lateral cartilages and the lower edge of the nasal bones is paramount. When the upper lateral cartilages are excessively resected or lose their support from the septum and nasal bones, they can collapse inwards. This inward collapse allows the caudal (lower) edges of the nasal bones to become visibly prominent through the skin, creating the characteristic inverted ‘V’ shadow. In 2026, advanced anatomical modeling and 3D simulation techniques are increasingly used in pre-operative planning to predict and prevent such structural imbalances, offering surgeons a clearer understanding of individual patient anatomy and potential post-surgical changes.- Nasal Bones: Form the upper third of the nasal dorsum.
- Upper Lateral Cartilages (ULCs): Form the middle third of the nose, connecting to the nasal bones superiorly and the septum medially.
- Nasal Septum: The central cartilaginous wall supporting the nose.
- Middle Nasal Valve: The narrowest part of the nasal airway, supported by the ULCs and septum; its collapse leads to both aesthetic and functional issues.
- Mechanism: Disruption of ULC support, often after dorsal hump removal, causes inward collapse and visibility of nasal bone edges.
Identifying the Signs: Symptoms and Diagnostic Criteria for Inverted-V Deformity
Recognizing Inverted-V Deformity involves assessing both its visual manifestations and the functional complaints reported by the patient. Early and accurate diagnosis is critical for effective treatment.İnverted V Deformity Visual Symptoms:
- Inverted ‘V’ Shadow: The most defining characteristic, a distinct shadow or indentation on the nasal bridge resembling an inverted ‘V’ when viewed from the front.
- Nasal Bridge Narrowing: A noticeable constriction or “pinched” appearance in the middle third of the nose.
- Supratip Deformity: Sometimes accompanied by an overly projected or “pollybeak” appearance of the area just above the nasal tip, or an overly rotated tip.
- Irregular Dorsal Contour: A lack of smooth, continuous lines from the brow to the nasal tip.
İnverted V Deformity Functional Symptoms:
- Nasal Airway Obstruction: Difficulty breathing through the nose, especially during physical exertion or while lying down.
- Chronic Nasal Congestion: Persistent feeling of stuffiness.
- Snoring and Sleep Disturbances: Due to compromised airflow, leading to reduced sleep quality.
- Mouth Breathing: Increased tendency to breathe through the mouth, particularly at night.
Patient Complaints:
- Aesthetic Dissatisfaction: Patients often express unhappiness with the unnatural or operated appearance of their nose.
- Reduced Quality of Life: Due to breathing difficulties, sleep disturbances, and self-consciousness about their appearance.
- Social Anxiety: Feelings of embarrassment or self-consciousness regarding their nasal appearance.c
Root Causes: Why Does Inverted-V Deformity Occur After Rhinoplasty?
The Inverted-V Deformity is primarily a consequence of specific surgical decisions and anatomical responses during or after a primary rhinoplasty. Understanding these root causes is crucial for both prevention and effective revision.- Excessive Resection of Dorsal Hump:
- Explanation: Over-removal of the nasal bones and/or upper lateral cartilages during dorsal hump reduction can destabilize the middle vault, leading to its collapse.
- Inadequate Support for the Middle Vault:
- Explanation: Failure to use spreader grafts or other supporting techniques after dorsal reduction leaves the upper lateral cartilages without sufficient lateral support, causing them to collapse inwards.
- Scar Tissue Contracture:
- Explanation: The natural healing process can sometimes lead to excessive scar tissue formation and contraction, pulling the nasal structures inwards and exacerbating the deformity over time.
- Surgeon’s Experience and Technique:
- Explanation: A lack of experience in rhinoplasty, particularly in understanding the delicate balance of nasal structures, can lead to aggressive resection or insufficient reconstruction. The choice of surgical technique (e.g., traditional vs. preservation rhinoplasty) significantly impacts the risk.
- Unfavorable Healing Process:
- Explanation: Individual patient healing characteristics, such as thin skin or pre-existing weak cartilage, can make them more susceptible to the deformity even with optimal surgical technique.
Prevention is Key: Strategies to Avoid Inverted-V Deformity in Primary Rhinoplasty
Preventing Inverted-V Deformity begins long before the surgery, with careful planning and the selection of an experienced surgeon. The goal is to maintain or restore the structural integrity of the nasal midvault during the primary rhinoplasty.- Choosing an Experienced Surgeon:
- Benefit: A board-certified plastic surgeon or ENT specialist with extensive experience in rhinoplasty, particularly with a deep understanding of nasal anatomy and advanced techniques, is crucial. Their expertise minimizes the risk of over-resection and ensures proper structural support.
- Detailed Preoperative Planning:
- Benefit: Comprehensive assessment of nasal anatomy, skin thickness, cartilage strength, and patient goals. 3D imaging and simulation tools, common in 2026, allow for precise surgical planning and prediction of outcomes, helping to identify potential risks.
- Conservative Cartilage and Bone Resection:
- Benefit: Avoiding aggressive removal of the dorsal hump, especially the upper lateral cartilages and nasal bones, helps preserve the natural support of the middle vault. The principle is to remove the minimum necessary tissue to achieve the desired aesthetic.
- Proactive Use of Spreader Grafts:
- Benefit: Spreader grafts, small pieces of cartilage placed between the septum and the upper lateral cartilages, are the gold standard for maintaining middle vault width and preventing collapse. They are routinely used during dorsal hump reduction to reconstruct the internal nasal valve and ensure adequate airflow.
- Adoption of Preservation Rhinoplasty Techniques:
- Benefit: Modern approaches like preservation rhinoplasty, which are gaining significant traction in 2026, focus on modifying the nasal dorsum from below (push-down or let-down techniques) rather than removing tissue from above. This preserves the natural dorsal aesthetic lines and the structural connections of the upper lateral cartilages, inherently reducing the risk of Inverted-V Deformity.
Advanced Treatment Approaches for Inverted-V Deformity
Correcting an Inverted-V Deformity almost always necessitates revision rhinoplasty, as non-surgical options offer only temporary and limited cosmetic improvements without addressing the underlying structural issues. In 2026, treatment focuses on restoring both aesthetic harmony and functional breathing through precise surgical reconstruction, often incorporating advanced imaging and personalized graft designs. Each case is unique, requiring a highly individualized approach based on the specific anatomical deficiencies and patient goals.Surgical Correction: Revision Rhinoplasty Techniques
Revision rhinoplasty is the primary and most effective treatment for Inverted-V Deformity. The goal is to reconstruct the middle vault, restore proper nasal contour, and improve nasal airflow.- Open vs. Closed Revision Rhinoplasty:
- Open Approach: Involves a small incision across the columella, allowing the surgeon direct visualization and precise manipulation of nasal structures. This is often preferred for complex revision cases like Inverted-V Deformity due to the need for intricate reconstruction.
- Closed Approach: All incisions are made inside the nose. While less invasive, it offers limited visibility and is generally reserved for less complex revisions or specific surgeon preferences.
- Middle Vault Reconstruction:
- Technique: The core of the correction involves re-establishing the structural integrity of the middle vault. This typically means separating the collapsed upper lateral cartilages from the septum and repositioning them laterally.
- Objective: To widen the internal nasal valve, improve breathing, and eliminate the inverted ‘V’ shadow by creating a smooth dorsal line.
- Cartilage Graft Sources:
- Septal Cartilage: Often the first choice if available, as it is readily accessible and has ideal stiffness.
- Ear (Conchal) Cartilage: More pliable, suitable for camouflage grafts or when septal cartilage is insufficient.
- Rib (Costal) Cartilage: Used for more extensive reconstructions, especially in cases requiring significant structural support or when septal and ear cartilage are depleted. Autologous (patient’s own) rib cartilage is generally preferred over cadaveric or synthetic options due to lower rejection rates and better long-term integration.
- Surgical Goals:
- Aesthetic Improvement: Eliminating the inverted ‘V’ shadow, restoring a smooth and natural dorsal aesthetic line, and correcting any associated irregularities.
- Functional Improvement: Widening the internal nasal valve to alleviate nasal obstruction and improve breathing.
The Role of Spreader Grafts and Camouflage Grafts
Grafts are fundamental to correcting Inverted-V Deformity, playing distinct but complementary roles in restoring both structure and aesthetics.- Spreader Grafts:
- Definition: Small, rectangular strips of cartilage placed between the dorsal septum and the upper lateral cartilages.
- Placement Techniques: Can be placed unilaterally or bilaterally, either internal (between the septum and ULCs) or external (on top of the ULCs).
- Role in Middle Vault Support: They act as internal splints, pushing the upper lateral cartilages outwards, thereby widening the internal nasal valve and preventing their inward collapse.
- Airway Improvement: Crucially, spreader grafts improve nasal airflow by expanding the narrowest part of the airway.
- Aesthetic Impact: They restore a smooth dorsal aesthetic line, eliminating the inverted ‘V’ shadow.
- Material Choice (2026): Patient’s own cartilage (septal, ear, or rib) is overwhelmingly preferred due to its natural integration and reduced risk of complications. Advanced graft shaping techniques allow for precise customization.
- Camouflage Grafts:
- Definition: Thin, finely diced, or crushed cartilage grafts used to soften irregularities, fill minor depressions, or smooth contours.
- Aesthetic Correction: Primarily used to mask visible edges, minor asymmetries, or subtle depressions that might remain after structural reconstruction. They create a smoother transition and more refined appearance.
- Material Options: Often made from ear cartilage or residual septal/rib cartilage, sometimes combined with fascia (e.g., temporalis fascia) for a softer, more natural feel.
Non-Surgical Adjuncts and Considerations
While surgical intervention is the definitive treatment for Inverted-V Deformity, non-surgical methods may be considered for very mild cases or as temporary aesthetic adjuncts. However, their limitations are significant and must be clearly understood.- Dermal Fillers (e.g., Hyaluronic Acid):
- Limited Use: Can temporarily camouflage the inverted ‘V’ shadow by filling in the depressions adjacent to the prominent nasal bones.
- Temporary Effects: Results typically last 6-18 months, requiring repeated treatments.
- No Structural Correction: Fillers do not address the underlying structural collapse of the middle vault or improve nasal breathing. They merely mask the aesthetic symptom.
- Potential Risks: Includes infection, vascular compromise, skin necrosis, and granuloma formation. Misplaced fillers can worsen the appearance or cause serious complications.
- Not a Surgical Alternative: It is crucial to emphasize that fillers are not a substitute for revision rhinoplasty in cases of true Inverted-V Deformity, especially when functional impairment is present.
- Misleading Claims (2026):
- In the current landscape of 2026, patients should be wary of misleading claims regarding “non-surgical nose jobs” as a permanent solution for structural deformities like Inverted-V. While they offer temporary aesthetic tweaks, they cannot rebuild collapsed cartilage or improve airflow.
Patient Journey: What to Expect During Diagnosis and Treatment
Navigating the process of diagnosis and treatment for Inverted-V Deformity can be a significant journey for patients. Understanding each stage helps manage expectations and promotes a smoother experience.- Initial Consultation:
- Detailed History: The surgeon will gather information about the patient’s original rhinoplasty, symptoms, and aesthetic concerns.
- Physical Examination: A thorough examination of the nose, both externally and internally (anterior rhinoscopy), to assess the deformity, nasal valve function, and overall nasal structure.
- Photo Analysis: Standardized photographs are taken from multiple angles to document the deformity and aid in surgical planning.
- Surgical Planning:
- Customized Approach: Based on the diagnosis, a personalized surgical plan is developed, often utilizing 3D imaging and simulation to visualize potential outcomes.
- Discussion of Grafts: The surgeon will discuss the type of grafts to be used (e.g., septal, ear, rib cartilage) and their role in reconstruction.
- Realistic Expectations: Setting clear, achievable goals and discussing potential limitations and risks of revision surgery.
- Anesthesia:
- Revision rhinoplasty is typically performed under general anesthesia to ensure patient comfort and safety throughout the procedure.
- Surgery Process:
- The procedure usually takes several hours, involving the precise placement of grafts and reshaping of nasal structures to correct the deformity and improve function.
- Immediate Post-Operative Period:
- Swelling and Bruising: Common around the eyes and nose, typically peaking within the first few days and gradually subsiding.
- Splint/Cast: An external splint or cast is usually applied to protect the nose and maintain its new shape, worn for about one week. Internal splints may also be used.
- Discomfort: Mild to moderate pain, managed with prescribed medication.
- Recovery Period:
- Initial Healing: Most significant swelling resolves within the first few weeks to months.
- Gradual Improvement: The final results become apparent as swelling fully dissipates, which can take up to 1-2 years.
- Activity Restrictions: Patients are advised to avoid strenuous activities, heavy lifting, and contact sports for several weeks.
- Long-Term Results and Follow-up:
- Regular follow-up appointments are crucial to monitor healing and assess the long-term aesthetic and functional outcomes.
- Emotional and Physical Challenges: Patients may experience emotional ups and downs during recovery. Realist expectations and support from family, friends, or even patient support groups (increasingly accessible via tele-health in 2026) are vital.
Choosing Your Surgeon: Expertise and Experience in Revision Rhinoplasty for Inverted-V Deformity
Selecting the right surgeon for revision rhinoplasty to correct an Inverted-V Deformity is arguably the most critical decision a patient will make. This complex procedure demands a high level of specialized skill, experience, and artistic vision.- Specialization and Board Certification:
- Importance: Ensure the surgeon is board-certified in plastic surgery or otolaryngology (ENT) with a sub-specialty focus on facial plastic and reconstructive surgery. Board certification indicates rigorous training and adherence to high standards.
- Extensive Revision Rhinoplasty Experience:
- Importance: Inverted-V Deformity correction is more challenging than primary rhinoplasty. The surgeon should have a significant track record specifically in revision cases, demonstrating proficiency in managing complex nasal anatomy and previous surgical alterations.
- Patient Reviews and Testimonials:
- Importance: Reviewing feedback from previous patients can offer insights into the surgeon’s communication style, patient care, and satisfaction with results. In 2026, reputable online platforms provide verified patient experiences.
- Before-and-After Photo Gallery:
- Importance: A comprehensive portfolio of before-and-after photos, particularly of revision rhinoplasty cases involving Inverted-V Deformity, allows you to assess the surgeon’s aesthetic style and technical capabilities. Look for natural-looking, balanced results.
- Communication Skills and Patient Rapport:
- Importance: The surgeon should be an excellent listener, capable of understanding your concerns, explaining the procedure clearly, and setting realistic expectations. A strong, trusting relationship is vital for a successful outcome.
- Facility Accreditation:
- Importance: Ensure the surgical facility is accredited, meeting stringent safety and quality standards.
Living with the Outcome: Psychological Impact and Support
The journey through Inverted-V Deformity and its correction extends beyond the physical surgery, deeply impacting a patient’s psychological well-being. Addressing these emotional aspects is crucial for holistic recovery and satisfaction.- Addressing Aesthetic Concerns:
- Successful revision rhinoplasty can significantly alleviate the distress caused by the visible deformity, restoring self-confidence and improving body image.
- Impact of Functional Improvement on Quality of Life:
- Improved nasal breathing directly enhances sleep quality, physical activity, and overall comfort, leading to a substantial boost in daily living.
- Need for Psychological Support:
- Patients who have undergone a primary rhinoplasty that resulted in a deformity may experience anxiety, depression, or body dysmorphia. Professional psychological counseling can provide coping strategies and support throughout the revision process.
- Patience and Realistic Expectations:
- The full results of revision rhinoplasty can take up to two years to materialize as swelling completely resolves. Patience and maintaining realistic expectations are essential for managing the recovery period.
- Role of Patient Support Groups (2026):
- In 2026, online forums and tele-health platforms offer accessible support groups where patients can share experiences, receive encouragement, and feel less isolated. Connecting with others who understand the unique challenges of revision surgery can be profoundly beneficial.
Do I Have an Inverted V Deformity?
Many individuals contemplating the aesthetic and functional aspects of their nose find themselves scrutinizing their reflection, searching for answers to specific concerns. The “Inverted V Deformity” is a common post-rhinoplasty complication, though it can also arise from trauma or, rarely, be congenital. If you’re asking this question, you’re likely observing something specific about the contours of your nose that has prompted this inquiry. While only a qualified medical professional can provide a definitive diagnosis, this section aims to guide you through a detailed self-assessment process, highlighting the key visual and functional indicators associated with this particular nasal condition.Understanding the Visual Hallmarks: What to Look For
The Inverted V Deformity is primarily a visual diagnosis, characterized by a distinct aesthetic irregularity in the middle third of the nose. To conduct a thorough self-assessment, position yourself in front of a well-lit mirror and observe your nose from various angles:- Frontal View Scrutiny:
- The “Inverted V” Shadow: This is the most telling sign. Look for a distinct, inverted V-shaped shadow or indentation across the middle third of your nose, just above the tip and below the bridge. This shadow is formed by the collapse or sharp angulation of the upper lateral cartilages, which are no longer adequately supported by the underlying nasal bones or septum. The apex of the “V” typically points towards the nasal tip.
- Mid-Vault Narrowing: Observe if the middle third of your nose appears disproportionately narrow or “pinched” compared to the wider nasal bones above and the tip cartilages below. This narrowing contributes to the visual prominence of the inverted V.
- Asymmetry: Note if the deformity is more pronounced on one side than the other, leading to an uneven appearance of the middle vault.
- Skin Redundancy/Creasing: In some cases, the skin over the collapsed area may appear slightly loose or even show fine creases due to the underlying structural deficiency.
- Oblique and Profile Views:
- Dorsal Concavity: From a 45-degree oblique angle, you might notice a subtle concavity or depression in the middle third of the nasal dorsum, further emphasizing the structural deficit.
- Loss of Smooth Contour: A healthy nasal dorsum should present a relatively smooth, continuous line from the bridge to the tip. An Inverted V Deformity often disrupts this fluidity, creating an abrupt change in contour.
- Palpation (Gentle Touch):
- Gently run your finger along the bridge of your nose. You might feel a distinct step-off or depression in the area corresponding to the visual inverted V. This tactile sensation can confirm the underlying cartilaginous collapse.
Beyond Aesthetics: Functional Symptoms to Consider
While often aesthetically concerning, an Inverted V Deformity can also significantly impair nasal function, as the structural collapse compromises the internal nasal airway. Consider if you experience any of the following:- Nasal Obstruction/Difficulty Breathing: This is perhaps the most common functional complaint. The narrowing of the middle vault directly restricts airflow through the nasal passages. You might notice:
- Persistent feeling of a blocked or stuffy nose.
- Difficulty breathing through your nose, especially during physical exertion.
- Worsening of obstruction when lying down or during sleep.
- A positive Cottle’s maneuver: If gently pulling your cheek skin outwards (away from your nose) temporarily improves your breathing, it suggests an external valve collapse, which is often associated with the Inverted V.
- Chronic Congestion: A constant sensation of fullness or blockage within the nasal passages.
- Crusting and Dryness: Altered airflow patterns can lead to increased dryness and crusting inside the nose.
- Recurrent Sinus Infections: Impaired drainage due to obstruction can predispose individuals to sinus issues.
- Snoring and Sleep Disturbances: Significant nasal obstruction can contribute to or worsen snoring and, in severe cases, may be a factor in obstructive sleep apnea.
- Headaches or Facial Pressure: Chronic nasal obstruction can sometimes lead to secondary headaches or a feeling of pressure in the face.
Reflecting on Your History: Potential Causes
Understanding the potential origins of an Inverted V Deformity can further inform your self-assessment:- Previous Rhinoplasty: This is by far the most common cause. If you’ve had a nose job, especially one involving aggressive dorsal hump reduction without adequate reconstruction or support of the middle vault (e.g., spreader grafts), you are at higher risk. The deformity may become apparent months or even years after the initial surgery as scar tissue contracts and unsupported cartilages collapse.
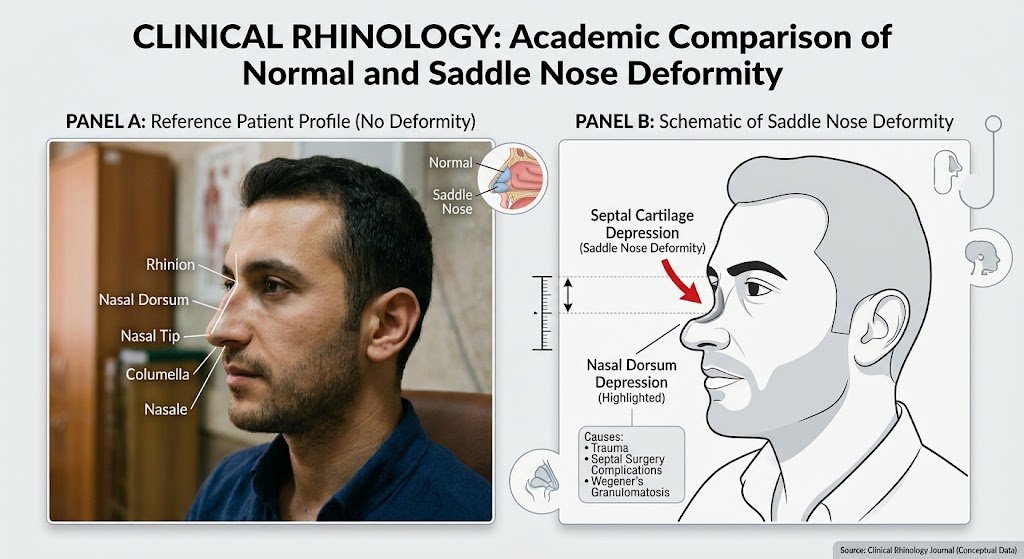
- Nasal Trauma: A significant injury to the nose that resulted in a fracture or displacement of the nasal bones and/or cartilages, particularly if not properly reduced or supported during healing, can lead to this deformity.
- Congenital Factors: While rare, some individuals may be born with weaker or abnormally shaped upper lateral cartilages that predispose them to an Inverted V appearance.
When to Seek Professional Consultation
If, after this detailed self-assessment, you recognize several of the visual and/or functional indicators described above, it is highly recommended to schedule a consultation with a board-certified facial plastic surgeon or an Otolaryngologist (ENT specialist) with expertise in reconstructive nasal surgery. They will conduct a thorough physical examination, including an internal assessment of your nasal passages, and discuss your medical and surgical history to provide an accurate diagnosis. They can differentiate an Inverted V Deformity from other nasal issues like septal deviation or turbinate hypertrophy, which can also cause breathing difficulties but require different treatment approaches. Remember, self-assessment is a valuable first step, but a professional evaluation is crucial for confirming the condition and exploring appropriate treatment options. If you are experiencing issues with inverted v deformity, you can contact the expert team at Faceaesthetics, specialists in revision rhinoplasty in Turkey.Frequently Asked Questions
No, Inverted-V Deformity is a structural issue caused by cartilage collapse and bone prominence. It will not resolve on its own and typically requires surgical intervention to correct.
Revision rhinoplasty is a complex procedure, often taking 3-5 hours, sometimes longer, depending on the extent of the deformity and the reconstructive work required.
Initial recovery involves swelling, bruising, and wearing a splint for about a week. Significant swelling subsides within a few months, but final results can take 1-2 years as all residual swelling resolves. Most patients can return to light activities within 2-3 weeks.
The cost of revision rhinoplasty for Inverted-V Deformity varies significantly based on the surgeon’s fees, anesthesia costs, facility fees, and the complexity of the case. In 2026, costs typically range from $8,000 to $20,000 or more. It’s essential to get a detailed quote during your consultation. Insurance coverage for the functional component (breathing improvement) may be possible, but the aesthetic component is generally not covered.
Non-surgical options like dermal fillers can temporarily camouflage the aesthetic appearance of a very mild Inverted-V Deformity. However, they do not correct the underlying structural collapse or improve breathing and are not a permanent solution. Surgical revision is the definitive treatment.
It is generally recommended to wait at least 12-18 months after primary rhinoplasty before considering revision surgery. This allows sufficient time for all swelling to resolve and scar tissue to mature, providing the surgeon with a stable and accurate
Inverted-V Deformity is a recognized post-rhinoplasty complication characterized by a visible inverted ‘V’ shaped shadow or indentation on the middle third of the nasal bridge. This aesthetic concern is often accompanied by significant functional issues, as it signifies a structural collapse of the nasal midvault. Visually, patients notice a pinched appearance and irregular dorsal contour, while functionally, it leads to nasal airway obstruction, difficulty breathing, and potentially snoring due to the narrowing of the internal nasal valve.
The deformity arises from a disruption in the delicate balance between the nasal bones, upper lateral cartilages (ULCs), and the nasal septum, which together form the middle nasal vault. Specifically, when the ULCs are excessively resected or lose their crucial support from the septum and nasal bones during primary rhinoplasty, they can collapse inwards. This inward collapse then allows the lower edges of the nasal bones to become visibly prominent through the skin, creating the characteristic inverted ‘V’ shadow and compromising the nasal airway.
In addition to the distinct inverted ‘V’ shadow, patients may experience nasal bridge narrowing, an irregular dorsal contour, and sometimes a supratip deformity. Functionally, common indicators include chronic nasal congestion, difficulty breathing through the nose (especially during physical exertion or while lying down), snoring, and an increased tendency for mouth breathing. In 2026, a definitive diagnosis requires a comprehensive evaluation by a board-certified plastic surgeon or ENT specialist, including an objective assessment like anterior rhinoscopy to visualize the internal nasal valve, alongside a thorough review of the patient’s aesthetic and functional complaints.
The primary surgical factors contributing to Inverted-V Deformity include excessive resection of the dorsal hump, which can destabilize the middle vault, and inadequate support for the upper lateral cartilages after dorsal reduction. If spreader grafts or other supporting techniques are not appropriately utilized, the cartilages lack sufficient lateral support and can collapse inwards. Furthermore, the surgeon’s experience and chosen technique play a critical role, as aggressive resection or insufficient reconstruction due to a lack of understanding of nasal anatomy can significantly increase the risk.
Preventing Inverted-V Deformity primarily involves careful planning and selecting a highly experienced surgeon for the primary rhinoplasty. Patients should seek a board-certified plastic surgeon or ENT specialist with extensive experience in rhinoplasty and a deep understanding of nasal anatomy and advanced techniques, as their expertise minimizes the risk of over-resection and ensures proper structural support. Additionally, detailed preoperative planning, which in 2026 often includes advanced 3D imaging and simulation tools, is crucial for precisely assessing nasal anatomy and predicting outcomes, thereby reducing the likelihood of this complication.
Inverted-V Deformity is frequently mislabeled as simply a “bad nose job” because its visible aesthetic flaw, the inverted ‘V’ shadow, is immediately apparent. However, this perception overlooks the underlying anatomical collapse of the nasal midvault and its significant functional consequences. Beyond cosmetic dissatisfaction, the condition often leads to compromised nasal airflow, causing difficulty breathing, chronic congestion, and sleep disturbances, thus impacting a patient’s overall quality of life.
In 2026, advanced technologies like 3D anatomical modeling and simulation tools are crucial for both understanding and preventing Inverted-V Deformity. These tools allow surgeons to conduct precise preoperative planning by visualizing individual patient anatomy in detail, predicting potential post-surgical structural changes, and identifying areas of risk. This enhanced insight helps surgeons make more informed decisions, ensuring the structural integrity of the nasal midvault is maintained or adequately supported during primary rhinoplasty

 (1)")